
The Mathematics of the Covid Vaccines By Brian Simpson
The establishment holds to the faith that Covid-19 vaccines will end the “pandemic.” Then we can get back to doing capitalist things, realising the true meaning of life. But, one of the challenges to this, as the US CDC admits, is virus evolution. Vaccines will set the virus off mutating to overcome this, which it may. But, apart from that biological arms race, there are intrinsic problems reaching herd immunity.
https://www.statnews.com/2021/02/10/vaccines-alone-wont-end-pandemic/
“I’m sorry to be writing the words that follow, but here they are: We can’t vaccinate our way out of this pandemic. And the myopic focus on achieving herd immunity through mass vaccination may even make it tougher for America — and the world — to defeat Covid-19.
Don’t get me wrong: Mass vaccination is essential. But herd immunity is a numbers game. It is defined as the point at which community spread of a disease stops because unprotected individuals are surrounded by a “herd” of people who are immune to infection, making it difficult, if not impossible, for infected people to pass on the disease.
Many experts have said we will achieve herd immunity when about 70% of the population is immune to SARS-CoV-2, the virus that causes Covid-19, either through vaccination or by having had Covid-19.
How do we reach that number?
It’s harder than it seems. For starters, while the Pfizer/BioNTech and Moderna vaccines showed about 95% efficacy in the clinical trials, vaccine effectiveness — how well a vaccine performs under real-world conditions — is likely to be lower for several reasons. One is that the people who participate in clinical trials are an imperfect representation of the whole population. They tend to be healthier, and younger. Real-world factors such as vaccine transportation and storage can also reduce vaccine effectiveness.
Say the Moderna and Pfizer vaccines now being given across the country achieve 90% effectiveness. Vaccinating 70% of U.S. residents puts us at 63% immunity. So, we’ll need to vaccinate a full 80% of the population to reach the herd immunity threshold.
Additional vaccines are starting to be approved. Some of them have lower efficacy. For instance, the AstraZeneca vaccine has about 70% efficacy, and Johnson & Johnson has reported that its one-dose vaccine has 66% efficacy. Their real-world performance could be lower still. If these vaccines become part of the mix in the U.S., actual protection will be lower than the estimated 90% we’d get from just the Moderna and Pfizer vaccines.
There are other barriers to achieving herd immunity. Vaccine uptake — how many people actually get vaccinated — is far below the level we need, in part because Covid-19 beliefs have been politicized in the U.S. and a percentage of the population doesn’t even believe the disease is real. In a Kaiser Health News survey released near the end of January, 13% of Americans said they would “definitely not” get vaccinated, 7% would take the vaccine only if it was “required,” and another 31% would “wait and see how it’s working” before getting vaccinated. Not encouraging numbers for those hoping for a quick journey to herd immunity.
Even when ample vaccine supplies are restored — perhaps by President Biden invoking the Defense Production Act — other factors will further drive down the number of people who get vaccinated. Eligibility factors currently exclude approximately 25% of U.S. residents from Covid-19 vaccination. The Pfizer vaccine can be administered only to those age 16 and up; for the Moderna vaccine, it’s those 18 and up. This represents approximately 20% of the population. Furthermore, although the CDC says that pregnant people may get vaccinated, it stops short of a clear recommendation. The decision is a “personal choice” left up to individuals and their health care providers.
Excluding those currently ineligible for vaccination against SARS-CoV-2 due to age or other conditions leaves 75% of Americans with no restrictions on vaccination. Factoring in the 13% of Americans who definitely don’t want the vaccine and the 7% who would get it only if it was required means just 49.5% of Americans would have immunity in the near future. If half of those who are in a wait-and-see mode don’t get vaccinated — another 15% of the population — then we are looking at just 40% vaccine coverage of the currently eligible population, far below the 70% needed for herd immunity. And that’s even before considering that real-world vaccine effectiveness will be below clinical trial levels.
The young people who aren’t cleared to get the Moderna and Pfizer vaccines have proven to be highly efficient asymptomatic spreaders of Covid-19. Leaving this population unprotected will enable the disease to continue to spread widely.
Finally, we don’t yet know the durability of the immune response to the various vaccines. It may persist. Or it may wear off, leaving people vulnerable after they’ve been vaccinated and creating conditions for new outbreaks.
If my years of global health work on the HIV/AIDS epidemic has taught me anything, it’s that even the best laid plans can’t anticipate every challenge. To vaccinate 75% of the U.S. population, approximately 248 million people — that’s nearly 500 million doses — are needed. And it means we need to be vaccinating nearly 2 million people a day so all of them are immune by the fall of 2021. As I write this, we’re vaccinating only about 1 million people a day. At that pace, Reuters estimates it would take until April 2022 for 75% of Americans to receive at least their first vaccine dose.
And that’s only if everything goes well logistically (it won’t) and if there are no further mutations in SARS-CoV-2 that make combating it more difficult (there will be).
It’s time to stop promoting the myopic belief that the unrealistic goal of herd immunity can be achieved in 2021 and start looking to reinforcing all aspects of the health care response as we start to concede that Covid-19 will become an endemic disease that will continue to lurk in the population. For the foreseeable future, that means continued physical distancing; occupancy limits in restaurants and other retail establishments; replacement of physical menus with smart phone-based menus to prevent surface spread of the virus, and more.
We’ll also need to monitor people who have been vaccinated to gauge the durability of the immune system’s response and whether booster shots are necessary, as they are for tetanus and diphtheria. Finally, our nation’s public health infrastructure will need to be bolstered, putting in place new protocols to monitor for new variants of the virus as soon as they emerge.”
“In recent weeks, a number of signs have emerged indicating the COVID-19 injections cannot put an end to COVID-19 outbreaks. In the July 15 video report above, Dr. John Campbell reviews data coming out of the U.K. On a side note, I do not agree with everything Campbell says in this video, such as promoting mask wearing, for example. It’s his data review that is of interest here.
As noted in the video, as of July 15, 87.5% of the adult population in the U.K. had received one dose of COVID-19 “vaccine” and 67.1% had received two. Yet symptomatic cases among partially and fully “vaccinated” are now suddenly on the rise, with an average of 15,537 new infections a day being detected, a 40% increase from the week before.
Meanwhile, the daily average of new symptomatic cases among unvaccinated is 17,588, down 22% from the week before. This suggests the wave among unvaccinated has peaked and that natural herd immunity has set in, while “vaccinated” individuals are becoming more prone to infection.
U.K. hospitals are confirming double-injected patients are part of the patient population being treated for active COVID infection, and two cities have issued public warnings to their residents, letting them know they may end up in the hospital even if they’ve been double-injected against COVID-19.
“There are currently 15 patients in hospital with COVID across the Trust; last month there were none,” The Yorkshire Post reported July 9. An undisclosed number of them had received two doses of COVID “vaccine.”
“The message I would like to share with you all is that some of their patients are double vaccinated,” Heather McNair, chief nurse at York and Scarborough Teaching Hospitals, told the Post.
“This is a disease that can still affect you and still make you poorly when you are double vaccinated. We have got a ward at the moment full of COVID patients in our hospital and that is not going away anytime soon.”
While the number of hospitalized COVID patients doubled in a single week, the total number was still well below the number reported in January — a statistic Amanda Bloor, accountable officer for the NHS North Yorkshire Clinical Commissioning Group, takes as proof that the injection program is “having the anticipated impact around reducing the risk of death and reducing serious illness.”
COVID surges in countries with highest injection rates
I wouldn’t be so quick to assume lower hospitalization rates in the middle of summer are a sign that the injections are having a positive impact. We also have data showing that countries with the highest COVID injection rates are also experiencing the greatest upsurges in cases, while countries with the lowest injection rates have the lowest caseloads. This trend “is worrying me quite a bit,” Dr. Robert Malone, inventor of the mRNA vaccine technology, said in a July 16 Tweet.
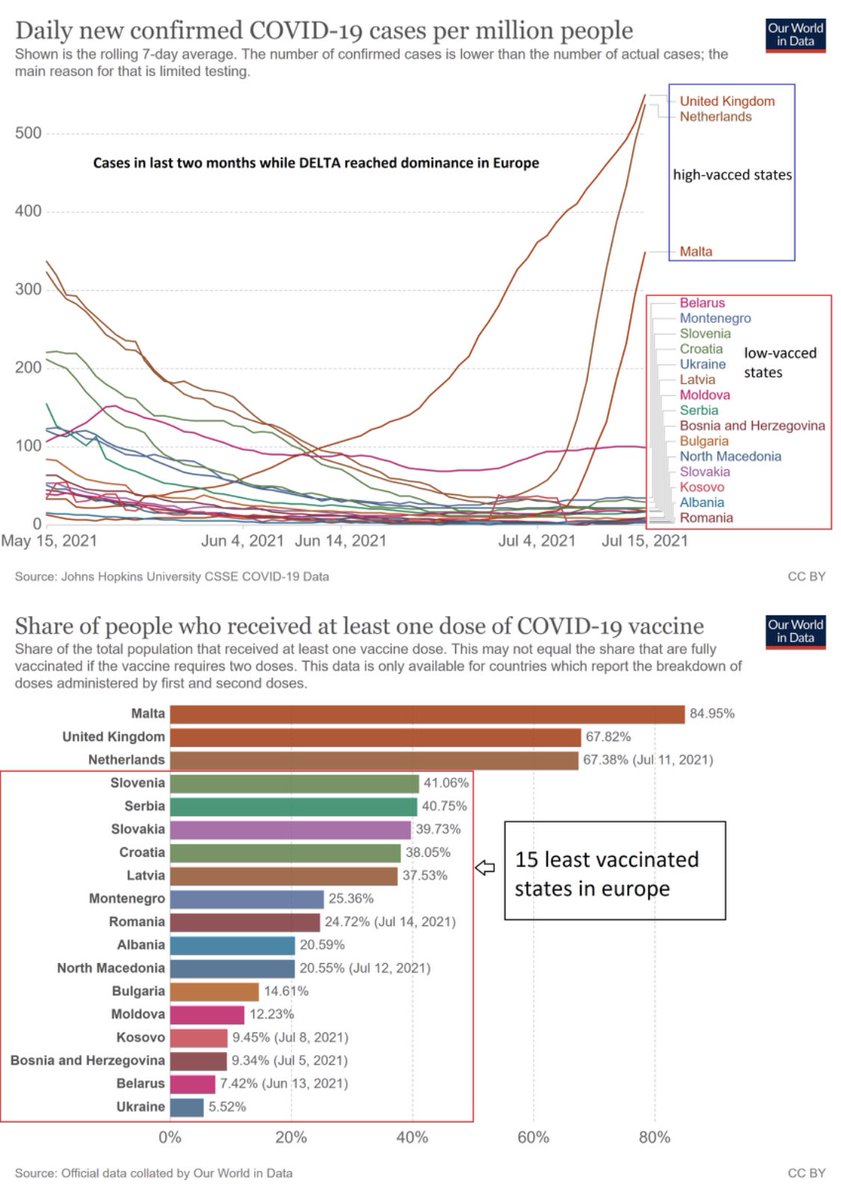{kind=link}
You can view more data in this thread, posted by Corona Realism. Cyprus, where more than 51% of residents have received the jab, now has the highest case count in the world. Interestingly, the outbreak on the British Navy ships — which I’ll cover further below — occurred shortly after a stopover in Cyprus.
Bhutan offers an interesting glimpse into the effects of mass COVID “vaccination”. They managed to get 64% of residents injected in just one week, starting March 27, and almost immediately, there was a rapid uptick in cases.
In the first graph below, you see the extraordinarily rapid injection rate in Bhutan, going from zero to 64% in a matter of days. In the second graph, you can see the effect on cases in the weeks that followed. They went from near-zero cases at the outset of the injection campaign, to a high of more than 400 cases per million in the weeks following.
On the flipside, we see the lowest number of positive COVID tests congregated in nations that also have the lowest rates of COVID “vaccine” uptake. While it’s not a 100% clear-cut correlation, it is a trend, and we also have to remember that the PCR tests have issues that complicate any attempt at data analysis.
The main problem is that if you run the PCR test at too-high a cycle threshold (CT), you end up with an inordinate number of false positives. The CT refers to the point in the test where a positive result is obtained. A CT of 35 or higher will give you a 97% false positive rate.
For maximum accuracy, you’d have to use a CT of 17. It’s unclear what all these countries are using, but it’s unlikely they’re using a CT below 20 as a matter of routine. This means most case counts around the world will be falsely elevated.
This is particularly true for unvaccinated individuals in the U.S., as their tests are recommended to be run at a CT of 40, whereas patients that have received a COVID injection will have their COVID tests run at a CT below 28. This makes it appear as though the case rate is higher among the unvaccinated, when in reality it’s just an artifact from highly biased testing and few of these falsely positive “cases” are actually sick.
Looking at the hospitalization rate for confirmed COVID-19 in the U.S., we see that the number of people sick enough to require medical attention is nowhere near what it was during the winter months of 2021, and since only 5.9% of American adults had been injected with two doses as of February 21, we can conclude that the injections did not cause this rapid decline in hospitalizations.
The best explanation for the decline in both cases and hospitalizations after the rollout of COVID shots is the emergence of natural herd immunity from previous infections.
In a July 12, 2021, STAT News article, Robert M. Kaplan, Professor Emeritus at the UCLA Fielding School of Public Health, calculated that by April 2021, the natural immunity rate was above 55% in 10 U.S. states, and in most of those same states, new infections were in rapid decline as early as the end of 2020, at a time when only a tiny fraction of the population had received their shots.
We must also remember that the U.S. Centers for Disease Control and Prevention are artificially driving down case rates, hospitalization rates and death rates for “vaccinated” Americans by selectively tracking breakthrough cases. They only track and report breakthrough cases where the patient is hospitalized or dies. They do not count mild cases, even if they have a positive test result.
A number of media outlets have expressed concerns about this biased tracking and reporting. As noted in Harvard Health, the CDC’s strategy prevents us from ascertaining whether one injection is more or less effective than another. It can also hide manufacturing problems and prevent us from determining whether timing of the second dose might have a bearing on effectiveness, as well as a number of other things.
Business Insider pointed out that not tracking all breakthrough cases makes it more difficult to determine how dangerous the Delta variant really is. NPR expresses a similar view, stating that “Critics argue the strategy could miss important information that could leave the U.S. vulnerable, including early signs of new variants that are better at outsmarting the vaccines.”
Even complete ‘vaccine’ coverage won’t stop infections
July 14, BBC News reported 100 fully injected crewmembers had tested positive onboard the British Defense aircraft carrier HMS Queen Elizabeth. It’s unclear whether any of them actually have symptoms. According to British defense secretary Ben Wallace, mitigation efforts include mask wearing, social distancing and a track and trace system. He made no mention of actual treatment for acute infection.
Other warships are also reporting onboard outbreaks, although Wallace did not offer any details about them. The fleet is currently in the Indian Ocean and plans to continue the 28-week deployment, with Japan as their destination. BBC News said the queen and prime minister had been onboard the flagship shortly before it sailed.
This case offers a sobering view into the effectiveness of these gene modifying shots, as the HMS Queen Elizabeth now has a case rate of 1 in 1620 — the highest case rate recorded so far, that I know of. Yet 100% of the crew has been double-injected. This tells you that the vaccine-induced herd immunity narrative is a fairytale. These injections apparently cannot prevent COVID-19 even if 100% of a given population gets them!
Israeli data indicate Pfizer ‘vaccine’ failure
Data from Israel also offer a dismal view of COVID-19 injections. Israel used Pfizer’s mRNA injection exclusively, so this gives us a good idea of its effectiveness. Overall, it looks like an abysmal failure, as a majority of serious cases and deaths are now occurring among those injected with two doses. The following is a screenshot of graphs posted on Twitter.
Overall, it doesn’t appear as though COVID-19 gene modification injections have the ability to effectively eliminate COVID-19 outbreaks, and this makes sense, seeing how it’s mathematically impossible for them to do so.
The four available COVID shots in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.22,23 (Efficacy rates of 67% to 95% all refer to the relative risk reduction.) Meanwhile, the noninstitutionalized infection fatality ratio across age groups is a mere 0.26%. Since the absolute risk that needs to be overcome is lower than the absolute risk reduction these injections can provide, mass vaccination simply cannot have a favorable impact.
CDC tries to hide COVID jab death toll
They can, however, cause unnecessary deaths among otherwise healthy individuals. Tragically, the CDC is doing everything it can to hide just how great that death toll is. In what appears to be a deliberate attempt at deception, the CDC “rolled back” its July 19 adverse events report to statistics from the previous week. I’ll explain. Take note of the specific dates and death totals in each of the following excerpts. The July 13 report reads as follows:
“Reports of death after COVID-19 vaccination are rare. More than 334 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through July 12, 2021. During this time, VAERS received 6,079 reports of death (0.0018%) among people who received a COVID-19 vaccine.”
The original July 19 report (saved on Wayback) initially read as follows:
“Reports of death after COVID-19 vaccination are rare. More than 338 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through July 19, 2021. During this time, VAERS received 12,313 reports of death (0.0036%) among people who received a COVID-19 vaccine.”
Please note, the death toll more than doubled in a single week. That original July 19 report was then changed to this. The date on the report is still July 19:
“Reports of death after COVID-19 vaccination are rare. More than 334 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through July 13, 2021. During this time, VAERS received 6,079 reports of death (0.0018%) among people who received a COVID-19 vaccine.”